When we look at girls with Rett syndrome we see that their movements have certain common characteristics:
And again: the same features, except the last one, are present in infants of 1-2-3-4 months of age.
I want to stress/emphasize here that this fact does NOT say anything about the intelligence of the child or about her cognitive potential. It only means that obstical which is blocking her normal development or is preventing therapeutic success, lays in that developmental stage. This obstruction is part of a reflexive behaviour which she can not overcome on her own. It is persistent and causes all other/later problems.
This point of view was an essential basis of our therapeutic approach. I saw that our biggest challenge lay in combining efforts to work on these four features parallel to our daily exercises. I tried to eliminate or at least reduce these features because I knew that as long as these (Rett) obstacles exist, there is no therapy that could have any success at all.
It is already well known that activating therapies do not show results with children that have Classical Rett syndrome. Why that is, is still an open question for the therapists. The very simple general opinion is that activating therapies fail because the affected girls can not learn and can not memorize. But I can only partly agree with that because: a learning difficulty is always a secondary symptom. It is never a problem on it's own but mainly the result of much deeper underling cause (like persistent immature reflexes in Rett syndrome). And talking about memory is even more complex.
One thing that I know for sure is that the memory is NOT significantly affected by this disease. As far as Dejana has/had a Classical Rett, and we have studied her reactions intensively, there were plenty of situations in which I saw that her memory is good enough but what she really misses is the possibility to learn from her own experience and environment. WHY is that so? Because she is passive, static and captured into the movement repetition that does not allow anything else in between.
Like most other girls she is not engaged in any voluntary physical action with her surroundings and toys because her constant reflexive stereotypes (mentioned above) are strongly preventing that. Since her body is forced to make these uncontrolled basic movements all day long she can never come (on her own) into the next developmental stage in which a typical child learns to use his/her own body parts to manipulate objects (9-24 months).
Girls with Classical Rett syndrome are therefore not aware of:
- their arms, legs, neck, feet, fingers, shoulders, hip, ears, tongue ... etc
- relations between the objects around them (inside, under, on each other... etc)
- how to use hands to manipulate an object (open the door, close the coat...etc)
Example:
We tried to teach Dejana to put blocks in a basket one by one. To do this she had to understand that the basket is an object with a hole in it. In other words she had to learn to see it in three dimensions. To realize that it has an edge and a surface. If she puts the block on the edge it will fall on the table, not in the basket... etc. The block has to be grasped with her hand and lifted high enough. She has to move it to the top of the basket and to release it in there. During all this time she has to follow the whole action smoothly with her eyes. As well she has to learn to control her arm and not allow her reflexes to interfere. There are a lot of body-object relations that she had to experience physically to be able to understand them !!!! But once she understood these basic principles she never forgot what she had to do in the same situation. Her actions are not RANDOM any more (like before). She learned how to do her actions: first by experiencing them: and then she memorized them. Her long term and short term memory were both active.



And the same happened with the other basic exercises. Once she understands them well she memorizes them easily. Children cannot learn these basic things just by watching them. Just like we can not learn to ski by watching the videos about it. She has to do it (HERSELF) on her own and to understand/learn through her own mistakes. After that memorizing will not be a problem. That was my surprising experience with Dejana.
Important to mention:
Dejana had a good memory mainly with the things that she can experience through the body. The things that she only looked at she memorized less well (like photos, books, symbols) which makes me believe that the first learning stage is a physically based process and the second learning stage includes looking/reading/listening too. But our girls are simply not ready for the second learning stage. It explains why the communication therapy has poor results in the Classical Rett syndrome. And it also explains why some specialists think that the memory is obstructed in this disorder. I am happy to say that while I was writing this text a molecular research about memory in Rett syndrome was just announced. It says that the long term memory is intact in this neurological disorder:
| RELATED RESEARCH: Intact long-term potentiation but reduced connectivity between neocortical layer 5 pyramidal neurons in a mouse model of Rett syndrome. Dani VS, Nelson SB. Biology Department, Brandeis University Waltham, Massachusetts,USA. Mutations in MECP2 cause Rett syndrome and some related forms of mental retardation and autism. Mecp2-null mice exhibit symptoms reminiscent of Rett syndrome including deficits in learning. Previous reports demonstrated impaired long-term potentiation (LTP) in slices of symptomatic Mecp2-null mice, and decreased excitatory neurotransmission, but the causal relationship between these phenomena is unclear. Reduced plasticity could lead to altered transmission, or reduced excitatory transmission could alter the ability to induce LTP. To help distinguish these possibilities, we compared LTP induction and baseline synaptic transmission at synapses between layer 5 cortical pyramidal neurons in slices of wild-type and Mecp2-null mice. Paired recordings reveal that LTP induction mechanisms are intact in Mecp2-null connections, even after the onset of symptoms. However, fewer connections were found in Mecp2-null mice and individual connections were weaker. These data suggest that loss of MeCP2 function reduces excitatory synaptic connectivity and that this precedes deficits in plasticity. Getting a Read on Rett Syndrome Greg Miller, 8 December 2006 Neuroscience �Greenberg says: In his view, the emerging picture of Rett syndrome suggests a breakdown of what neuroscientists call experience-dependent plasticity. The earliest stage of brain development, in which neurons form their initial connections, proceed largely according to genetic plans. In later stages, neuronal activity triggered by (an animal's) interactions with its environment fine-tunes neuronal connections, strengthening effective synapses and weeding out ineffective ones. Early life experience literally alters the brain's wiring, and Greenberg suspects that MeCP2 plays a key role in this process by regulating genes such as BDNF.... etc.It's no coincidence, he says, that the onset of Rett syndrome happens at about 1 year of age, a time when experience-dependent plasticity is in full swing in the human brain....� |
MAIN STEREOTYPES
As we already know, the process of understanding = learning is the challenging point in the Classical Rett syndrome. Early learning that is based on self experience is difficult for these girls because of persistent engagement of their mind/brain in the body stereotypes. Nothing else can come through. Therefore I completely focused myself on that problem. As a result I noticed that Dejana and all other Rett girls that I ever saw had TWO stereotype circles:
1 ___ shoulder/arm/hand repetitive movements
2 ___ jaw/tongue/repetition as a part of the breathing-sucking-swallowing disco ordination.According to the Neuro-developmental therapies: it shows over-activity (immaturity) of the Brain Stem and low brain centres.
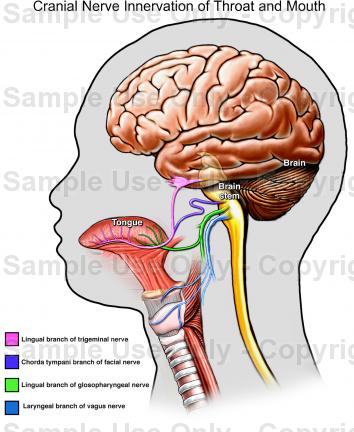
It is already a generally adopted view that the key symptom of the Classical Rett syndrome is a hand repetition. But I found out that Dejana�s �hand� stereotype involves more than just her hands and fingers, in fact, this is only one part of the much broader process. The stereotype also involves strong repetitive movement of the shoulders and arms and it is all connected with a forced tension in the jaw, tongue and breathing-swallowing�sucking reflexes !!!! All 12 Cranial nerves are involved in it as well. In fact, this is the (reflexive) stage of a young infant who is learning to establish a balance between:
This is important to consider if we want to design a good therapy-activating program.
Jaw/Tongue/Throat stereotype loop
It is obvious that most of the girls with CLASSICAL Rett syndrome have visible tension in the jaw/mouth and stereotype of the tongue. But it is strange that this fact was not mentioned in the list of the Rett symptoms. In fact we found out that this area may be the KEY problem in whole disorder. Why?
Her basic life functions are not fully established. They are still in the reflexive and uncoordinated stage and it does not seem that she can overcome this on her own. Instead she is locked into the repetitive movements of the small muscles of: tong, palate, esophagus, jaw opening/closing, jaw switched to one side, or forward, mouth and lips stretched� etc.
Most of them I could feel with my hands and fingers when I started to work on diminishing her general tension in this area. Of course some of them could only be felt through the skin of her neck and throat, like those of esophagus or the base of the tongue. It is not only tension that I noticed there but also the reflexes of repetitive sucking, or swallowing, combined with the hyper ventilation, turning of the tongue and sometimes I could feel the (high frequency) tremor too. Some of the muscles can stay in spasm and then we see that the girl's face looks like a mask or has a rigid smile.
Hick-ups, screaming, fanatic biting, uncontrolled drooling, teeth grinding, difficulties with drinking and eating, gag reflex, esophageal reflux and breathing problems are all part of the same problem. The cause is: an immature sucking, swallowing and breathing pattern. These internal movements are present during all her waking hours and become her main activity. These movements are also present in the young infant, but here they tend to normalize within the first months of life. All these activities are not voluntary and they are controlled by the lower brain centers. She can not influence this, but it will restrict her in her daily activity.
| RELATED ARTICLES: The Nervous System: The Ultimate Athlete Amy Venditta: spring 2005 ...In a newborn baby, the motor cortex area of the brain is not completely developed. This is why a newborn baby's movement is limited to sucking, swallowing, and breathing. As the motor cortex area, or motor strip, within the brain begins to develop, the baby is able to perform simple gross movements, such as lifting the head.... etc. ebsco.smartimagebase.com/imagescooked/14228W.jpg The EARLIEST RELATIONSHIP T. Berry, Brazeton M.D. Craner M.D. CHAPTER: Feeding Behavior Sucking is made possible by the thorax when the infant breathes in and by fixing the jaw between breaths. Swallowing and breathing must be coordinated, and the depth and rate of breathing are handled differently when the baby is engaged in nutritive and non-nutritive sucking (such as on fingers or a pacifier). In the latter, the chance of inhaling milk is not important. This whole process has been studied by Albrecht Peiper who argues for a hierarchical control system in which swallowing controls sucking and sucking controls breathing (Peiper, 1963). There appear to be three components of sucking: One can feel all three of these by putting a finger in the new baby's mouth. There is a brief delay before these become coordinated in an effective drinking/eating/breathing mechanism. CHAPTER: Sucking and gagging reflexes Initially, newborn babies need to rid themselves of the mucus in their airways. At this point, gagging reflexes compete with sucking. As a result, a baby's response to a nipple or finger will often be to gag and spit up before he or she can begin to suck. The sucking reflex must be gradually brought out and reinforced. Learning to suck is the baby's task. Coordination of breathing, sucking, and swallowing during bottle feedings in human infants J. S. Koenig, A. M. Davies and B. T. Thach Edward Mallinckrodt, Washington University School of Medicine, Children's Hospital St. Louis, Missouri 63110. In coordination of sucking, swallowing, and breathing might lead to the decreased ventilation that accompanies bottle feeding in infants, but the precise temporal relationship between these events has not been established. Therefore, we studied the coordination of sucks, swallows, and breaths in healthy infants (8 full-term and 5 pre-term). Respiratory movements and airflow were recorded as were sucks and swallows (intra oral and intra pharyngeal pressure). Sucks did not interrupt breathing or decrease minute ventilation during non-nutritive sucking. Minute ventilation during bottle feedings was inversely related to swallow frequency, with elimination of ventilation as the swallowing frequency approached 1.4/s. Swallows were associated with a 600-ms period of decreased respiratory initiation and with a period of airway closure lasting 530 +/- 9.8 (SE) ms. Occasional periods of prolonged airway closure were observed in all infants during feedings. Respiratory efforts during airway closure (obstructed breaths) were common. The present findings indicate that the decreased ventilation observed during bottle feedings is primarily a consequence of airway closure associated with the act of swallowing, whereas the decreased ventilatory efforts result from respiratory inhibition during swallows. ARTICLE: Normal breathing Inspiration is the process of taking in a breath, while expiration is the process of breathing the air out. Inspiration involves three groups of muscles: Expiration mostly occurs passively (the chest that has expanded during inspiration gradually falls back to the starting point before inspiration), but forceful expiration involves the use of abdominal muscles. For example, a cough is a forceful expiration and requires contraction of the abdominal muscles. The diaphragm is supplied by nerves that come from the spinal cord at the levels C3, C4, and C5. The external intercostal muscles are supplied by nerves T1 through T11. For example, the T1 nerve supplies the intercostal muscles between the ribs T1 and T2. The T10 nerve supplies the intercostal muscles between the ribs T10 and T11. Some of the accessory muscles such as the trapezes are supplied by cranial nerves that come from the brain stem. The abdominal muscles are supplied by nerves from T6 through L1. Ventilation is the mechanics of breathing in and out. When you inhale, muscles in the chest wall contract, lifting the ribs and pulling them, outward. The diaphragm at this time moves downward enlarging the chest cavity. Reduced air pressure in the lungs causes air to enter the lungs. Exhaling reverses theses steps. ARTICLE:�Vagus nerve Source: www.neurologychannel.com/vagus/ Vagus nerve stimulation involves the implantation of a generator that stimulates the vagus nerve and thus reduces seizure activity. The vagus nerve is one of 12 pairs of cranial nerves (i.e. nerves that originate in the brain). It has motor functions in the larynx (voice box), diaphragm, stomach, and heart, and sensory functions in the ears and tongue. It has both motor and sensory functions in the pharynx (sinuses) and esophagus. Stimulation of the vagus nerve is thought to affect some of its connections to areas in the brain that are prone to seizure activity. |
{kind=link}
Summary: There fore I strongly believe that breathing irregularity in the Rett syndrome can not be distinguished from the biting/sucking/swallowing process and it can not be treated alone if we want to get any success in the therapies. It relates to the occupational as well as for the potential medical treatment.
Hands/Arms/Shoulders stereotype loop
Baby's play with their arms/hands in the same way but with TWO exceptions:
Kids with Rett syndrome only adopt one sequence of that complex play and they go on for years repeating that single form like the wheel of a car that keeps turning in one place in the mud. They do not even look at their hands. Every girl has her own pattern which she repeats over and over again all life long (according to Rett statistics).The stereotype will lessen only when she gets older and all her body movements slow down because of a passive life style or medication. But it is a negative rather than a positive development.


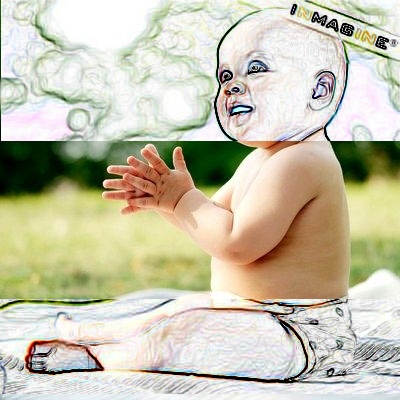



All photos presented here show infants with normal development engaged in �hand play�. None of them have Rett syndrome or other disorder. Baby may play with her hands and feet for a few minutes at a time. She's quite fond of doing one action over and over again (repetitive) until she's sure of the result. Then she'll switch things around to see what the new result is. Infants learn about their body and coordination from that play.
But a girl with Rett syndrome stays locked into only one repetitive form for the rest of her life. Also, she does not learn from this hand �play� like other babies. It is useless: it is not emotional, not protective, does not make her feel safe or calm. It is uncontrolled and forceful, many times occupying her entire nervous system and escalating into baiting and screaming spells. It also causes deformities in her arms and fingers. All in all this neurological �performance� is working against her and it would be good to find a way to get rid of it.
| RELATED RESEARCH: Repetitive behaviors in autistic disorder Militerni Roberto. Bravaccio Carmela, Fico Cinzia, Palermo Mark T. The Department of Child Neuropsychiatry, II University of Naples, Naples, ITALIE A recurrent suggestion for the developmental origins of aberrant stereotyped behaviors among persons with mental retardation proposes that such behaviors emerge or evolve from repetitive motor behaviors typical during infant development. This behavioral pattern resembled that of typical repetitive movements in infant development to such an extent that it was suggested that they have a similar etiology, neuro maturation, and share adaptive significance as discharge or displacement activities. Younger autistic children displayed more motor and sensory repetitive behaviours. Older children had more complex behaviours. Children with higher IQ scores, likewise, demonstrated more complex repetitive behaviours..... RELATED BOOKS about the normal development: Understanding Motor Development Gallahue, D.L. & Ozmun, J.C.. McGraw-Hill This book covers the entire lifespan. It focuses on the phases of motor development and provides a solid introduction to the biological, affective, cognitive, and behavioral aspects within each developmental stage. The reader is presented with the most up-to-date research and theory, while the Hourglass Model is used as a consistent conceptual framework that brings clarity to understanding infant, childhood, adolescent, and adult motor development. Important is Chapter 2: NORMAL Infant Reflexes and Rhythmical Stereotypes The study of infant reflexes and stereotypical patterns of behavior yields useful information for better understanding the process of motor development and designing therapies. Key Concept of this chapter are Rhythmical stereotypes. They are repetitive rhythmical movements normal in infants from 4 weeks � 1 year. Some of them include: These early rhytmical movements are an important precursor to motor skill development. But they were also found to persist in children with disabilities (Down syndrome, Tourette's syndrome, psychomotor retardation, blindness, deafness etc) |
can also be located in the well known Piglet's table (look at the marked section)
|
Developmental Stage & Approximate Age |
Characteristic Behavior |
|
|
|
|
Reflexive Stage |
Simple reflex activity such as grasping, sucking. ( SINGLE reflexes) |
|
Primary Circular Reactions |
Reflexive behaviors occur in stereotyped repetition such as opening and closing fingers repetitively. |
|
Secondary Circular Reactions |
Repetition of change actions to reproduce interesting consequences such as kicking one's feet to more a mobile suspended over the crib. |
|
Coordination of Secondary Reactions |
Responses become coordinated into more complex sequences. Actions take on an intentional character: the infant reaches behind a screen to find a hidden object. |
|
Tertiary Circular Reactions |
Discovery of new ways to produce the same consequence or obtain the same goal such as the infant may pull a pillow toward him in an attempt to get a toy resting on it. |
|
Invention of New Means Through Mental Combination |
Evidence of an internal representational system. Symbolizing the problem-solving sequence before actually responding. Deferred imitation. |
Repetitive behaviour is commonly found in autism, but also in other developmental disabilities.
Stereotype in the Classical Rett syndrome is completely neurological but it also shows which sensory pathways are the most immature by the specific/individual girl. That means that we can find out in which direction our therapy has to go and what our first goals should be. Several examples of repetitive behaviour are listed below and are not specifically related to the Rett syndrome.
rubbing face/hands, sucking on tongue (present in Rett syndrome too)
Scolioses and stereotype
In the Classical Rett syndrome scoliosis has a different origin. It is generally caused by: the body staying in a bad postion for hours, sitting in the wheel chair all day long, absence of physical activities, weak back muscles, tight muscles on one side... etc. But one of the very important triggers of the scoliosis is the arm/hand stereotype. Girls that can walk, or have enough exercise like Dejana, can also develop a curve in the spine despite the general belief that physical activity will prevent it. How is that possible?
Since their hand/arm stereotype is so persistent and strong (also during the therapy sessions) it is forcing the whole upper body to twist on one side. We can also see on the photos of almost all girls that their hands are never settled in the middle of the body, but always placed more to one side. This happens because of the dominant strength of one arm. I also saw with most of them that their shoulders were bent foreward or lifted up as part of arm-hand reflexive repetition.
On the other side I saw that girls who receive strong anti epileptic medication and become sedated by it, don't have suchstrong hand/arm/shoulders stereotypes and therefore also have less problems with scoliosis. Their body is generally more floppy . But the medication will cause other problems of course and I am not a fan of medication any way.
So, the girls that have stereotype all day will have high pressure on their spine for so may hours that the spine will start to curve. And if she does exercises WHILE her arm/hands are engaged in repetition, these exercises will not count. Physical therapy will only have effect on her spine if her arms are not involved in the stereotype during treatment. For us, that was one more reason to fight with her strong hand/arm repetition. We saw that each time she managed to stop the stereotype for some time, her torso and spine would return to a straight position because Dejana is still very flexible in her body.
It is also important to say that the curve of the spine in Classical Rett syndrome which develops in the first years of life is not always a permanent deformity. Even if we can not immediately correct her back with our hands or with a brace, the curve is not yet irreversible. This type of scoliosis is called: POSTURAL. The spine becomes so rigidly bent to one side because the muscles on that side become spastic and/or shorten. I am now talking about the deep layer of the muscles too. Therefore it is better to work on the muscles first, so that an operation can be delayed or maybe even avoided all together. Some parents are using Botox injections, but these only give a temporary effect. I am more in favor of physical activation and goal directed exercises. T his gives long term results. If a girl is left to sit in the passive and bad position for years; with strong arm/hand repetition, twisted to one side; and her back muscles become more and more spastic/tight; she has a big chance of developing a REAL STRUCTURAL scoliosis deformity... This involves bones as well as muscles and ligaments and an operation is the only treatment option but does not guarantee that the spine will stop deformation. I know parents whose children had twisting of the hip after the scoliosis operation. Their pediatricians explained that it was caused by the dystonia that is still present despite the fixation of the spine.
Fixation means the spine no longer bends but the tension still exist and goes down to the hip or up to the sholders deforming them instead. Therefore, in some cases, the scoliosis operation does not solve the problem at all. We are still fighting with Deajana's tendency for scoliosis. It originates from her arm/hand stereotype.
Scoliosis classification from the literature:
|
Spine curvature, without rotation, can be caused by following problems: "slipped" disc perhaps |
Congenital form develops (in utero) before birth. Acquired form develops after birth and includes: |
DYSTONIA ___ and movement disorders
There are various forms of movement disorders in Classical Rett syndrome. One example is ataxia, characterized by a lack of coordination while performing voluntary movements. The problem may appear as clumsiness, inaccuracy, or instability. Movements are not smooth and may appear disjointed or jerky. Another example is hypertonia, a condition marked by an abnormal increase in muscle tension and a reduced ability to stretch. Movement disorders almost always prevent the normal development of hand-eye coordination, learning from experience and voluntary action (all things necessary for the normal human development).
Some of the movement disorders often seen in Rett syndrome:
or to the cognition (you do not know WHAT to do with a certain object) This one is resent in the Classical Rett syndrome
But the most common disorder in the Classical Rett syndrome is Dystonia
TO BE CONTINUED