First of all it is important to say that I am talking here only about the Classical Rett syndrome. I am not talking about Atypical Rett where girls are functioning on much lower or higher levels. Atypical Rett syndrome is classified now in several categories and each of them has its own name and characteristics. The latest classification looks like this:
| Congenital variant | Classical Rett syndrome | Forme Frust | Zappella variant | Autism PDD-NOS | Normal functioning |
When I looked at girls in all these categories, on video or in real life, I noticed that they can all be placed at a specific step of the regular human development ladder. In fact, each of them stopped climbing this ladder at some point. It is easy to see that the girls in each consecutive Rett category achieved higher and higher skills, starting from the preterm borne baby to the normal functioning on the peer level.
I saw that the hand stereotype (repetitive movement) in the higher Rett variants becomes less dominant or does not exist at all. It also mimics the stages of a normal child development. There is one exception: the lowest Congenital variant. It also has a weak hand stereotype, but for a different reason. This variant is similar to a preterm borne infant and has a hypotonic body (weak muscles). All her movements are therefore diminished as is the hand/arm stereotype. The strongest arm/hand repetition is present in the Classical Rett syndrome just as in the infant during the first year of life.
I would now like to present table of normal development that (in my opinion) is similar to the Rett classification:
| Preterm borne - 3 mnt | Between 4-12 months | Between 1-2 years | Between 2-3 years | Above 3 years | Follows peer level |
I would say that:
Each girl with any Rett variant, has stopped somewhere on the scale of normal development. She can stay there for the rest of her life or we can try to move her to the next level by a strong stimulation program.This is how I see Rett syndrome from the therapeutic point of view. Once I adopted this approach, it became clear to me how I could redesign Dejana's therapy: first I determined on which step she was on the normal developmental ladder and then I started to work on the first following milestone that she hadn't yet achieved. We asked BIBIC (British Institute for Brain Injured Children) to assess Dejana's fine motor and gross motor skills, language and cognition. Each of these was on a different developmental level but not too far from each other. One workingday is too short to address all of these issues equally, I chose to put the focus on her fine motor and gross motor exercises. But I will explain this further in the section called: "Our Therapy".
A:
Developmental level does not show intelligence or the potential of a person. It only shows to what extent the brain has established control of the body (parts) and how mature the sensory system is. Using developmental skills to measure IQ is one more prejudice of old times. That was the main reason why special children (Rett) are often seen as unable to learn and very little effort is put into therapy with them. In fact it is rather that WE do not now HOW to teach them, than that they can not learn.
Normal child development = maturation of the brain
that gradually takes control of the body parts and movements.
The brain controls:
1- large movements = gross motor skills
2- precise movements of small muscles = fine motor skills
3- tongue, jaw and mouth = eating and speech . etc ....
Brain-motor development of the whole body is completed by 6 (7) years of age!!!
Gross motor development is 90% complete by two years of age!!!!
Fine motor skills are 60% developed by 5 years!!!!
OBSTACLES in CLASICAL RETT
To remind you: I am talking only about Classical Rett syndrome.
Before we started with developmental skill exercises I wanted to know what prevented Dejana from learning and developing in general. After a year of watching and comparing I discovered TWO main OBSTACLES which dominate her daily functioning and block her learning. I see them as the basic trigger of all other symptoms in this disorder:
|
(low brain function) I found out that Dejana’s stereotype is not based only on hands as it seems. Hands are only part of a larger process. Rett stereotype involves TWO main areas: 1- shoulders, arms and hands repetition 2- forced repetitive movements in the muscles of jaw, tongue and throat involved in the process of: breathing, swallowing and sucking |
(high brain function) Main reason for this is Ideation apraxia Definition: It is a disturbance of voluntary movement in which a person misuses objects because he/she has difficulty identifying the concept or purpose behind the objects. It is important to note that motor movement is not lost in ideation apraxia. It is about: |
On the basis of this view I adjusted our therapy program once more, to be able to deal with these issues. It is important to say that I had to work on both problems at the same time. Treating them one by one did not help.
I can also say: These are two main similarities that I recognize now in almost all girls with Classical Rett syndrome. When I watch them or their video's I see a clear system in this disorder. Their hand/arm/shoulder and jaw/mouth/tongue stereotype may have a different form (position) and may be of different strength but they are always present, during most of the day. Sometimes the stereotype movements are so slight that it becomes difficult to see during short observation and sometimes it is so strong that it turns into spasticity in the whole upper body. Within years, spasticity will slowly alter the stereotype and the body will become too rigid to move the arms and hands. Many people see this as neurological diminishing of stereotype but I would rather say that it is obstructed by increasing rigidity. The stereotype can also lessen due to anti epileptic medication which slows down all activities of the body and the brain (as well as the repetition.
REFLEXIVE MOVEMENTS (playing part in the second regression period)
It is very often seen in the Classical Rett syndrome that, within several years, girls slowly regress in motor skills, but it is also known that Rett is not a neuro-degenerative disease. On the other side research is showing that with exercise (if appropriate) a girl's condition can improve. We did a lot of exercises with Dejana but still she found it more and more difficult to walk when she reached the age of 10-11. Because I don't give up easily I wanted to know what was happening to her so that we could work on it more effectively and: as I discovered earlier the right therapy is essential for the good result.This is what I found out:
Her walking was always reflexive and never planned. She was not really aware of her legs, knees and feet: of their movements and their position (proprioception). She walked semi automatically as most of the girls with the Rett syndrome do. Even if it seems that they move with awareness they do it reflexively for the most of the time. Their proprioception has not yet developed. Reflexes are also present in the infants when they start to walk but at some moment they realize that they have legs for walking. They raise this awareness by stepping hard, suddenly changing direction, looking at their feet, catching them while sitting, kicking toy etc. After that period of discovery they will walk reflexively again for the rest of their lives but awareness of the legs will have been established. Most of the girls with a Classical Rett syndrome never pass through that developmental stage.
That is why they:
"The brain stem receives impulses from the senses in the head and body, it either reacts:
1 ___ directly to those impulses by creating a REFLEXIVE motor response,
2 ___ or relays the impulse to a higher center (cerebral hemispheres).
The majority of movement in the baby are automatic responses, generated by a collection of reflexes that come from the brain stem. These reflexes are called Primitive Reflexes This stimulus response action involves a simple sensory motor loop type of nerve pathway, It does not interact with the higher conscious brain and the reaction is always the same .... We know that babies develop in stages, each stage heralding more complex abilities and control as the brain matures and new wiring is laid down. These abilities and controls being a combination of more adult Postural Reflexes - generating from the mid brain and overriding many of the lower “Primitive Reflex reactions - and will add movements initiated by the higher conscious brain.....Failure within the mechanisms of development can result in a cluster of Primitive Reflex reactions remaining which will always undermine consciously movements from the higher regions of the brain ....."
Besides that: A reflexive walking that never becomes deliberate can not stay all life long. First of all, infantile reflexes are time limited and at some moment they start to diminish. Besides that, the legs and body become to big and to heavy (sometimes spastic) to be moved only by a reflex that moves a tiny baby. Girls that weigh 30- 40-50 kg start to walk slower and with more difficulty and we see that as the gross motor regression. Without exercise their bodies will become rigid and infantile reflexes will not help walking any more.That was my hypothesis.
Then I began to stimulate her awareness of the legs and I hoped that if she discovered them she would regain her walking. It took me almost two years and her walking has improved. I am sure now that the loss of walking has mainly to do with the problem of proprioception and lack of extremity awareness in Classical Rett syndrome. When the Primitive reflex of walking weakens she starts to lose her walking skills and we call it a second regression. We should work then mainly on her proprioception because balance may be better developed than we think.Reflexive movements are present in all body parts from head, face, arms, to the hips, legs and feet. For these girls reflexive movements are standing in their way to learning and making free voluntary actions. It can explain why girls with Rett syndrome are randomly performing correct actions especially if they do not think about them.
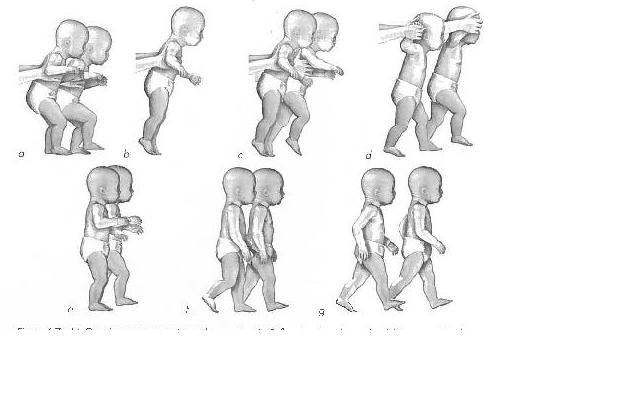
Picture above: McGraw's seven stages of erect locomotion. (A) reflex stepping phase; (B) inhibitory or static phase;
(C) transition phase which includes activities such as stomping of foot or stand bouncing and the reappearance of stepping movements; (D) deliberate stepping phase with erect posture; (E) independent stepping phase making the start of independent walking; (F) heel-toe walking; (G) adult pattern of walking with synchronous swinging of the arms with opposite leg
Consulted literature on this issue:
1- Infant motor development by Jan p. Piek
2- http://suehyland.co.uk/index.html
3- Neuro- developmental therapies,
SEPARATE MOVEMENTS and RETT
I have never seen a girl with the Rett syndrome who moves only one part of the body without moving lots of other parts at the same time. Even if they eat their whole body moves. Most of time they need to swing while they chew food. They do not have isolated movement. It disturbs their motor learning and because of that their brain can not focus on one action at the time. Motor learning is therefore almost impossible. That's why the most important part of our therapy with Dejana is preventing other extremities to move wile only one is active. By doing so we make it easier for her brain to establish only one correct pathway. Sometimes we need the assistance of two people to be able to exercise in a correct way. It is also very difficult for the girl (Classical Rett) to make an isolated movement, but in the end, she can succeed.
...... TO BE CONTINUED .....